There is a particular kind of institutional memory that forms not from deliberation but from desperation. It hardens quickly, the way bone does around a poorly set fracture, and it is extraordinarily resistant to correction once the original crisis has passed. The history of American medical policy is, in no small part, a history of this hardening — of provisional answers given under battlefield conditions that were later mistaken for settled science.
The psychological mechanism is not complicated, and it is not unique to medicine. When a society faces an overwhelming emergency, the first solution that appears to work acquires a sanctity that no subsequent evidence can easily dislodge. The men who administered that solution become its advocates. The institutions built around it become its defenders. And the patients who received it become, in the public imagination, its proof.
History did not need a randomized controlled trial to produce this pattern. It only needed human beings under pressure.
The Civil War and the Amputation Orthodoxy
The American Civil War produced approximately 620,000 deaths and something in the neighborhood of 400,000 wounded soldiers who required surgical intervention. The Union Army alone performed roughly 30,000 amputations. The Confederate medical corps, operating with fewer resources and less reliable supply chains, performed tens of thousands more.
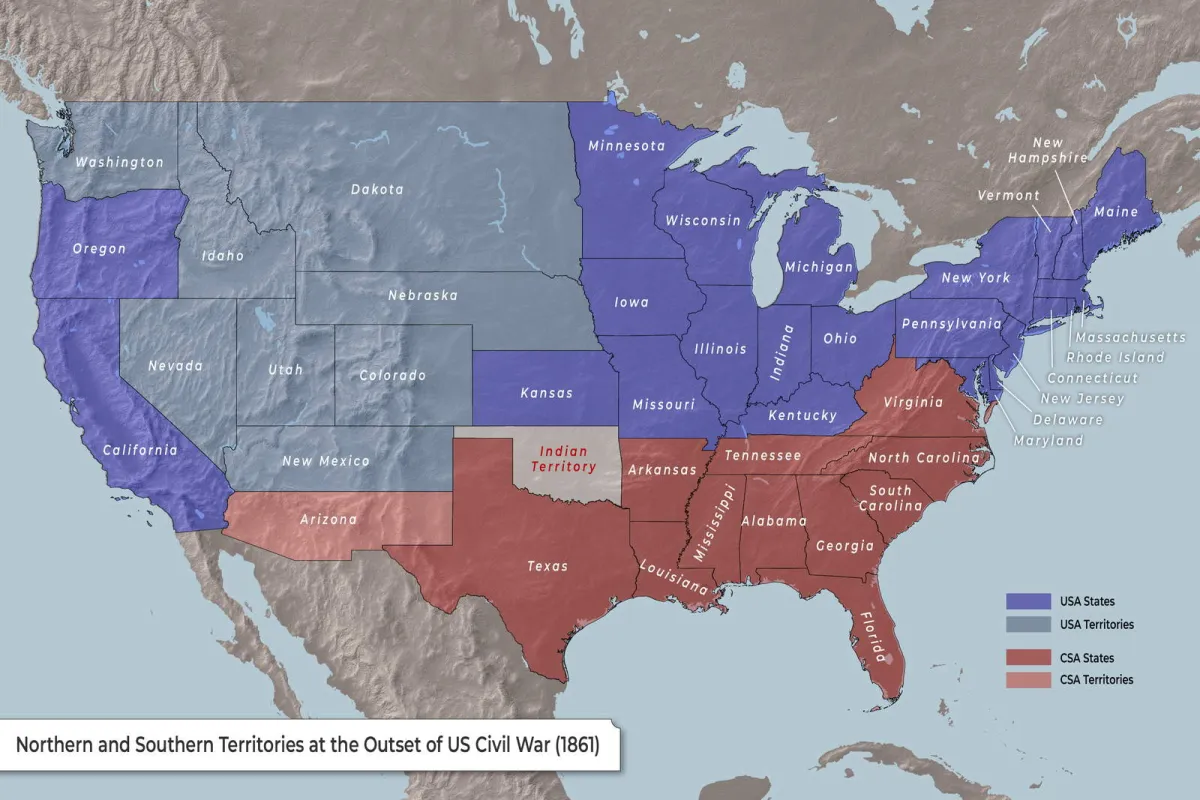 Photo: American Civil War, via cdn.thecollector.com
Photo: American Civil War, via cdn.thecollector.com
The surgeons who conducted these operations were working at the edge of what medicine understood. Anesthesia was newly available. Antiseptic technique was not yet standard — Lister's foundational work on carbolic acid would not appear until 1867. The primary concern of a battlefield surgeon in 1862 was not infection prevention but speed: a limb removed quickly was a soldier who survived the table. The statistics, such as they were, seemed to support the approach. Soldiers who underwent prompt amputation died at lower rates than those whose wounds were left to fester while surgeons deliberated.
What emerged from those four years of mass surgical practice was not merely a set of techniques. It was a codified doctrine, taught in the medical schools that trained the next generation of American physicians, embedded in the first systematic American surgical textbooks, and administered through the Veterans' Bureau and its successor institutions for decades afterward. The amputation protocols developed under the specific constraints of battlefield medicine — inadequate antiseptic knowledge, overwhelmed surgical teams, the genuine priority of speed over precision — were absorbed into peacetime practice as established wisdom.
The surgeons who challenged this orthodoxy in the 1880s and 1890s, arguing that many amputations had been unnecessary and that limb-salvage techniques deserved serious investigation, encountered the full weight of an institution that had organized itself around the wartime conclusion. They were not wrong. But they were inconvenient.
The Second World War and the Pharmaceutical Precedent
The federal regulatory machinery governing American pharmaceutical approvals was itself a product of crisis. The Food, Drug, and Cosmetic Act of 1938 had been passed in the aftermath of the sulfanilamide disaster, in which a poorly tested solvent killed over one hundred people. But the law's practical application was immediately complicated by the demands of a second world war.
 Photo: Second World War, via warfarehistorynetwork.com
Photo: Second World War, via warfarehistorynetwork.com
 Photo: Food, Drug, and Cosmetic Act, via image2.slideserve.com
Photo: Food, Drug, and Cosmetic Act, via image2.slideserve.com
The War Production Board, the Office of Scientific Research and Development, and the military services collectively created an approval environment in which the normal requirements for evidence were subordinated to the demands of supply. Penicillin, sulfa drugs, and antimalarials were produced and distributed under emergency authorizations that bypassed the deliberative processes the 1938 law had envisioned. The results, in terms of battlefield survival rates, were genuinely remarkable. American soldiers died of infected wounds at rates that would have been unimaginable in any previous conflict.
The institutional lesson absorbed from this success was not that emergency authorization had worked well under emergency conditions. The lesson absorbed was that faster approval produced better outcomes. The pharmaceutical industry, the military establishment, and significant portions of the medical community spent the following decades arguing — with the war as their evidence — that the deliberative process was itself the enemy of effective medicine.
This argument shaped every subsequent debate over drug approval timelines, from the thalidomide crisis of the early 1960s to the accelerated approval pathways created in the 1980s and 1990s. The wartime exception had become the baseline against which all subsequent standards were measured. Those who argued for more thorough pre-approval evidence were, in this framing, the ones departing from the norm — not the ones defending it.
The Psychological Architecture of Permanent Exceptions
What makes this pattern so durable is not institutional cynicism, though cynicism is certainly present. It is something more fundamental to human cognition: the tendency to measure all future performance against the first solution that appeared to work.
A surgeon who saved lives with rapid amputation in 1863 did not experience his technique as a compromise. He experienced it as a discovery. A pharmacologist who watched penicillin rescue soldiers from septicemia in 1944 did not understand accelerated approval as a concession to emergency. He understood it as proof that the old deliberative process had been unnecessarily cautious. These are not dishonest readings of experience. They are entirely natural ones. They are also, history suggests, dangerous ones when the conditions that justified the original approach have changed.
The men who built American medical institutions after each of these conflicts were not fools. Many of them were brilliant. But they were building on foundations poured under conditions of extreme pressure, and they rarely had sufficient distance from those conditions to evaluate them clearly. The students they trained had even less distance. The students those students trained had none at all.
What the Ledger Shows
The historical record does not suggest that wartime medical innovation was without value. It was, in many cases, genuinely transformative. The point is narrower and more troubling: the conditions under which wartime medicine operates — urgency, incomplete information, the overwhelming priority of short-term survival — are precisely the conditions least suited to producing standards appropriate for peacetime application.
Yet those standards have been produced, repeatedly, and defended with the full institutional authority of the establishments that inherited them. The provisional has become the permanent. The exception has become the rule. And the generations of patients who received the resulting care had no way of knowing that the protocols governing their treatment had been written, in the first instance, for men dying in fields.
History is not a warning that goes unheeded because people are foolish. It goes unheeded because the psychological mechanisms that produce these outcomes — the sanctification of the first working solution, the institutional defense of inherited doctrine, the framing of caution as obstruction — are not flaws in human cognition. They are features of it. Understanding that distinction is the beginning of doing better. The ledger has been keeping the record. The question is whether anyone is reading it.